Imaging
The COPDgene Study employs the use of CT imaging to help us accurately diagnose lung disease. Along with spirometry and genetic SNPs that may be associated with COPD, we aim to use CT data to re-characterize COPD phenotypes and elucidate a more complete picture of COPD.
As part of our commitment to this component of our study, in February 2010 we held a COPDGene CT Workshop at which over 400 CT scans from our cohort were scored by over 45 pulmonologists and radiologists from around the country. From this data we were able to submit four abstracts and one presentation for the Radiologist Society of North America conference.
CT Scan Use in COPD Diagnosis
In COPD, CT scans may be important for a variety of clinical reasons, particularly to identify other potential causes for symptoms of cough or breathlessness. Symptoms of COPD may be mimicked by other conditions such as bronchiectasis, chronic infection, lung fibrosis, and lung cancer, all of which can be detected by CT. CT is particularly important in patients with COPD who experience a change in their symptoms. In patients with severe COPD, CT provides useful information to help determine whether surgical treatment may be an appropriate option, and to identify parts of the lung that are suitable for resection1. While some have advocated use of CT for early detection of lung cancer, it remains unclear whether this will truly decrease the death rate from lung cancer. The ongoing National Lung Screening Trial should provide a definitive answer to this question.
Patients with COPD may have a wide spectrum of pulmonary abnormality on CT, ranging from pure emphysema to pure airway inflammation without emphysema. Indeed, people with identical degrees of disability from COPD may have very different amounts of emphysema. CT provides an extraordinary amount of information about the severity and distribution of emphysema and airways abnormality in COPD (see Figure 1). The clinical applications of this powerful tool are still not fully apparent, but it seems plausible that different treatments could be used for patients with predominant emphysema than for those with airways disease.
Early adoption of exciting new technology is not appropriate unless it has real benefit for the patient. Several ongoing research studies, such as the COPDGene study, will be critical in determining the value of CT in characterizing COPD.
In the COPDGene® Study, CT is being used as a tool to quantify the extent of emphysema, airway wall thickening and air trapping in individual patients, in order to correlate with the genetic markers. This novel use of CT is already providing important information regarding the structural abnormalities underlying COPD.
Radiation Risk from CT
CT scans are acquired using ionizing radiation. Exposure to ionizing radiation may cause some increase in risk of cancer. The precise level of risk is not known, but appears relatively small. For example, in a 57 year old female smoker, the estimated lung-cancer risk from the radiation from a COPD CT scan is about 0.05%, or 1 in 2,000. Nonetheless, it is important to minimize any risk. Because CT may be associated with a small increased risk of cancer, CT should be performed only where this risk is outweighed by potential clinical benefit, or in the context of an approved research study. The CT scans should be performed with the lowest possible radiation exposure.
CT Examples and Analysis
There are many ways in which CT scans are used to view lungs. Different aspects of a lung can be evaluated from the same CT scan by using computer software. Several examples of how CT scans can be used to view the lungs are shown below.

Figure 1. An axial image from a smoking control subject. Axial images look at a cross-section of a lung for signes of disease or abnormality. This image displays no evidence of emphysema, but there is centrilobular nodularity indicating smoking-related respiratory bronchiolitis.
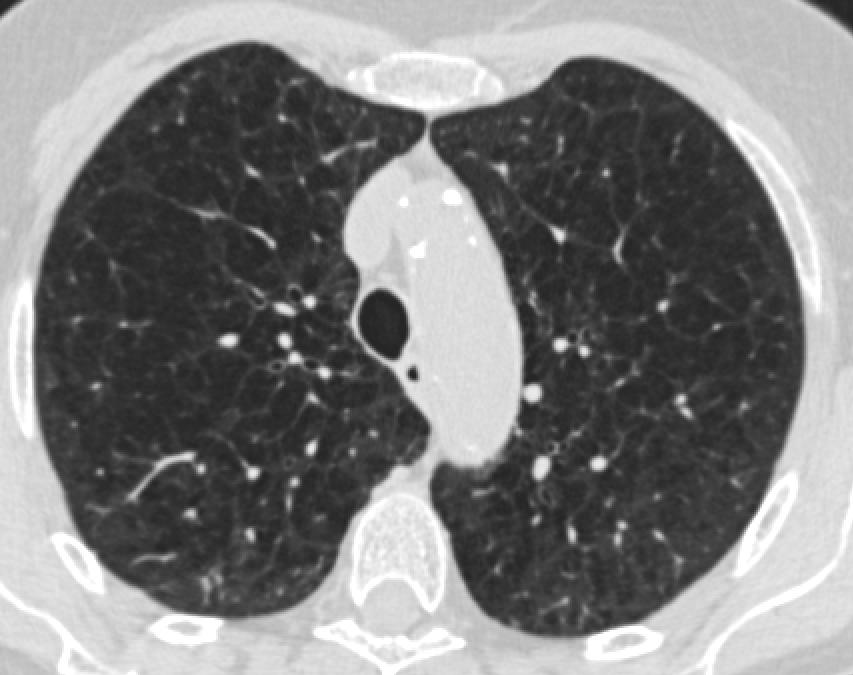
Figure 2. An axial image from a COPD GOLD stage 1 subject. The image displays early signs of centrilobular emphysema.
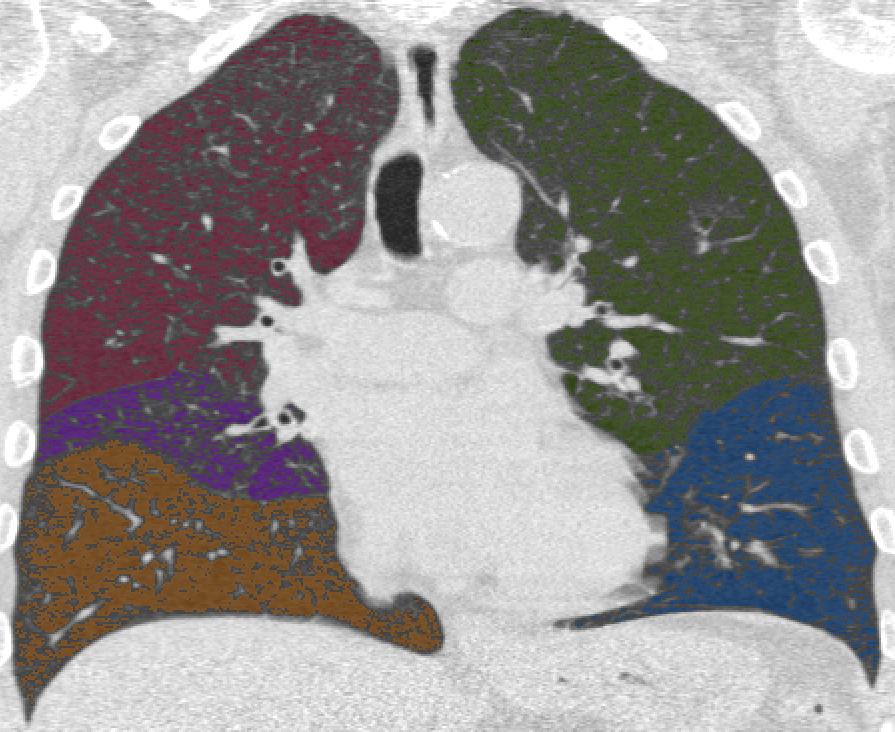
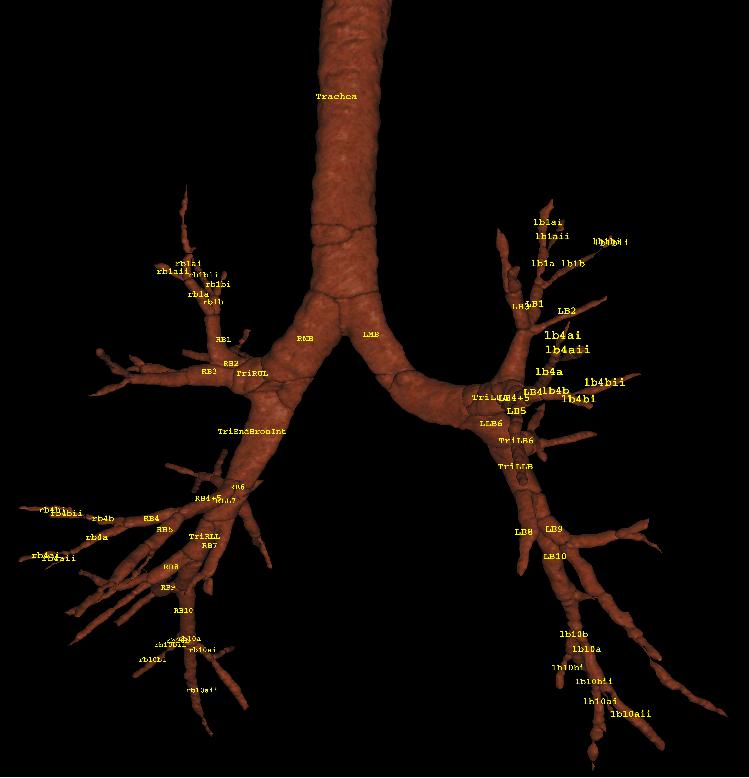
Figure 4. A 3-D representation of an airway tree. When lung tissue is removed from view on a CT scan, the bronchial tree or part of the lung that conducts air can be visualized. An airway tree can be 'traced' with computer software to get an idea of airway health. The figure above is labeled with six pathways traced for quantification.
